
The Vitamin That Makes Chemotherapy Deadly
April 21, 2026
Don’t Shake the Vial
May 1, 2026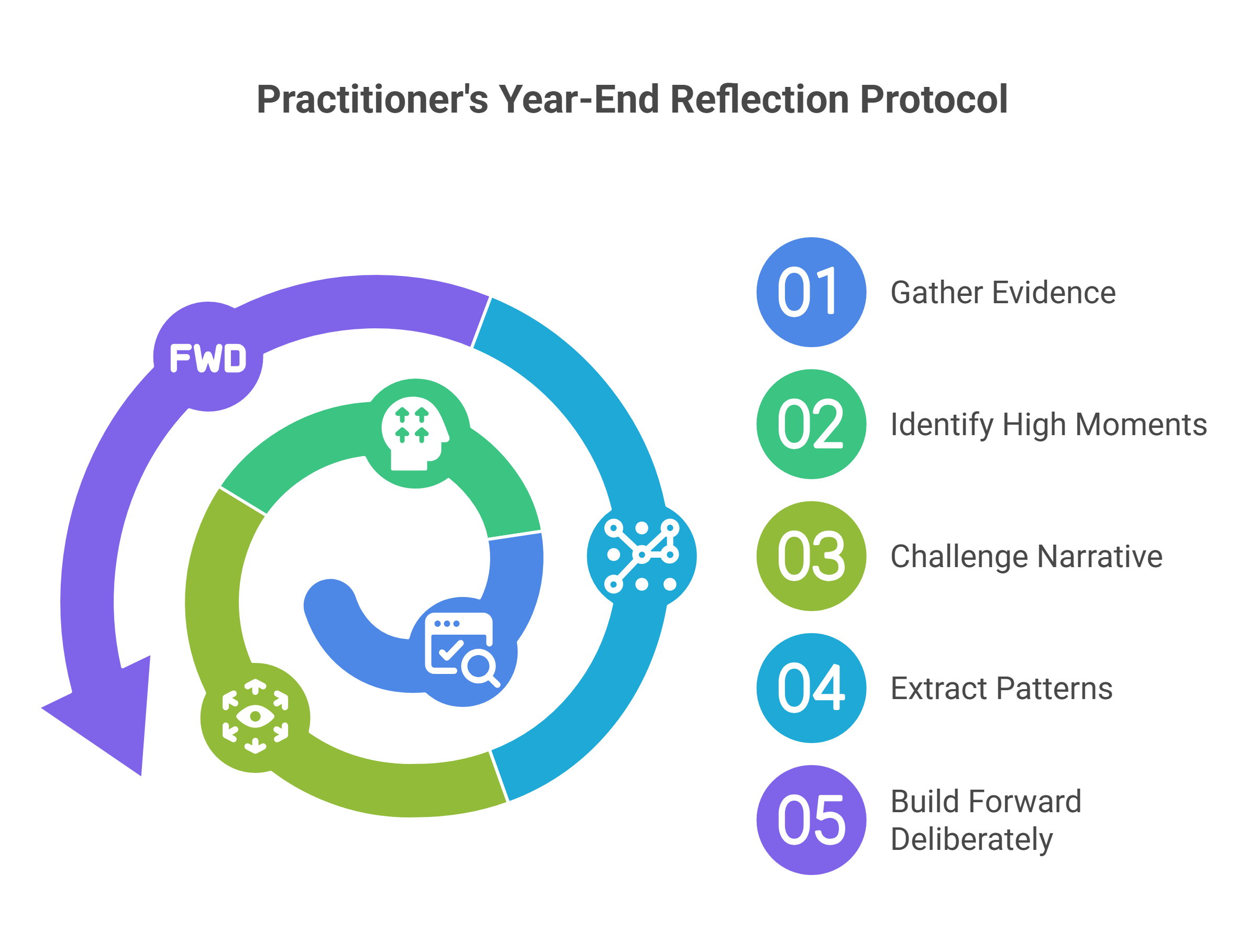
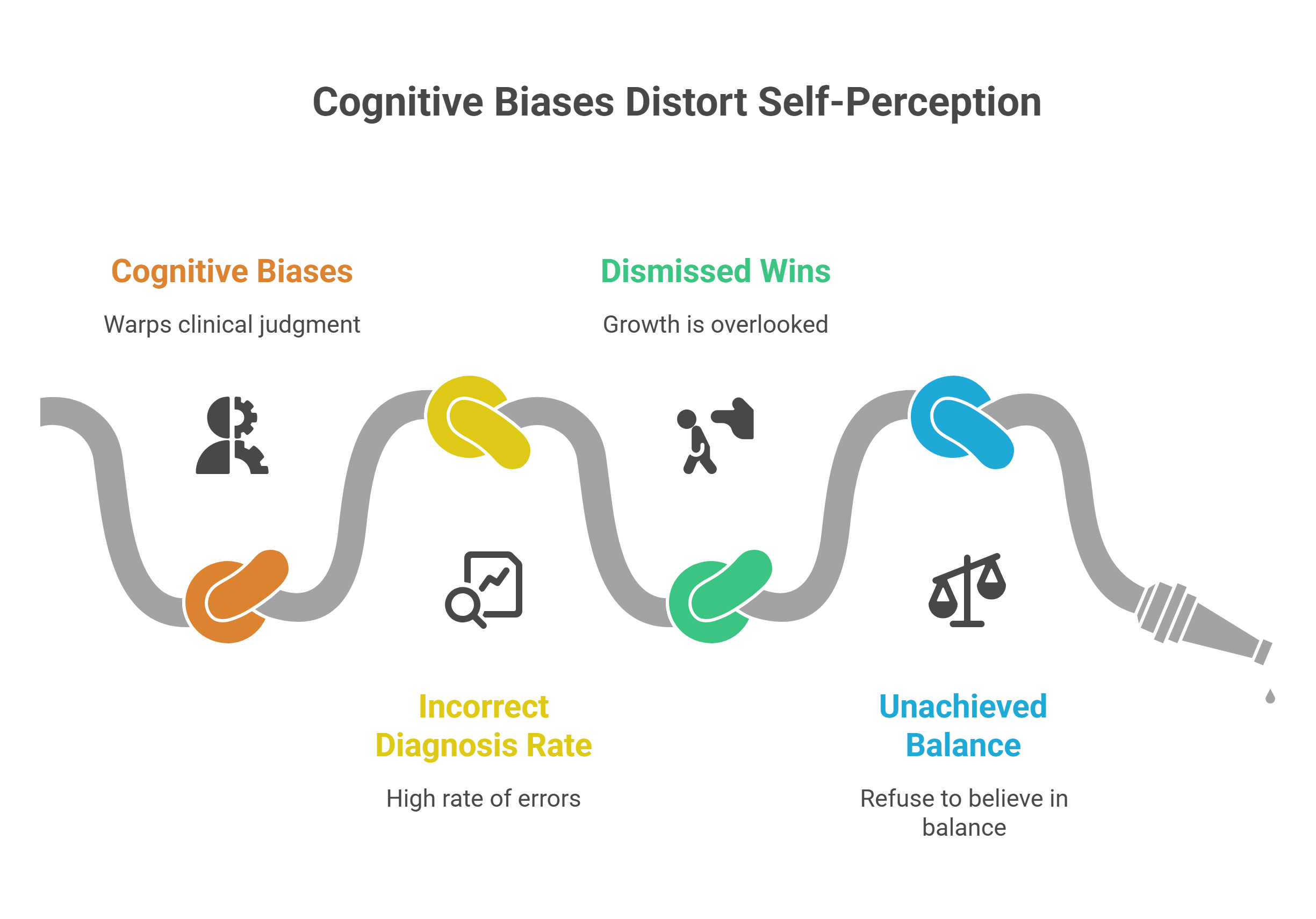
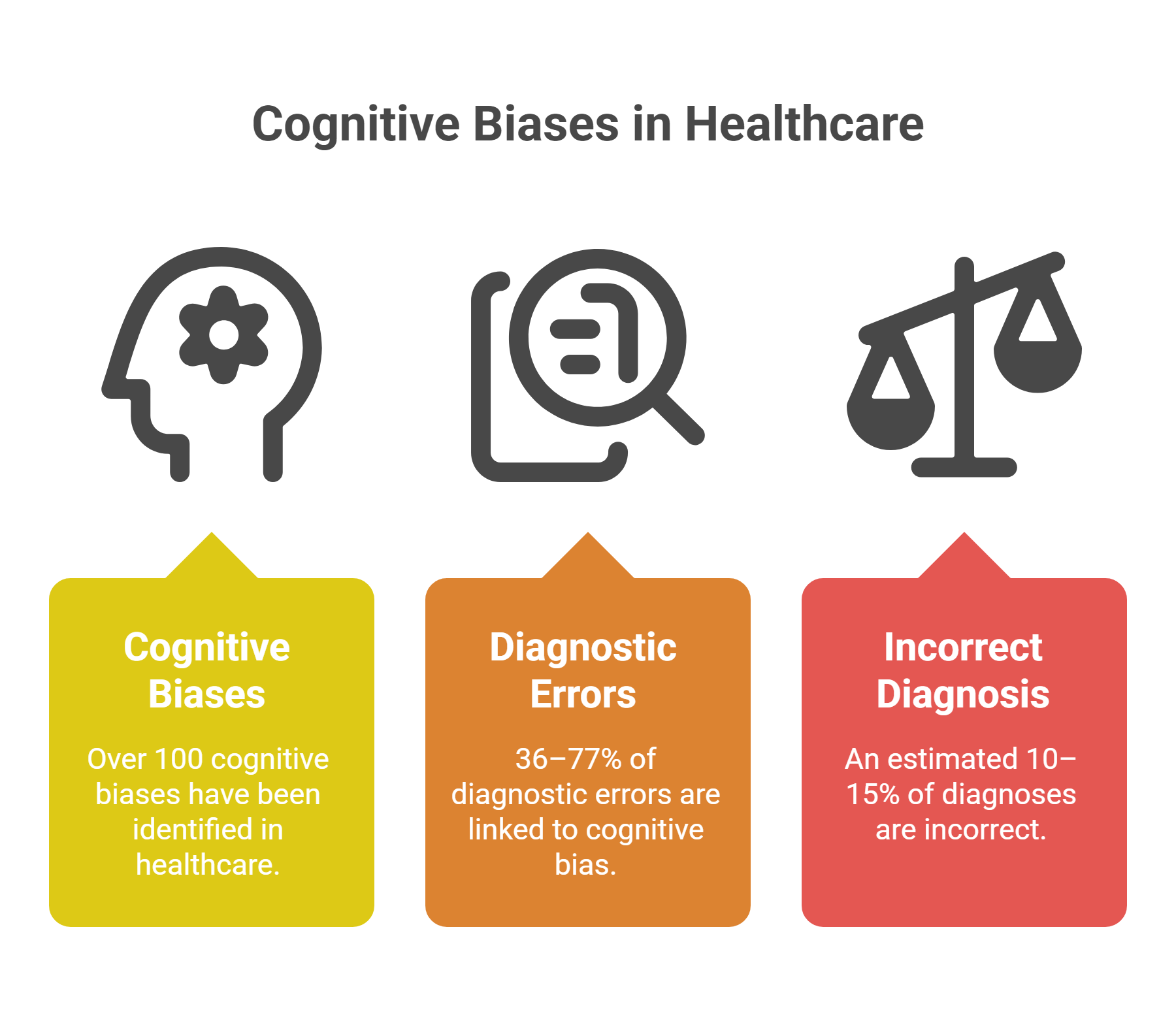
More than 100 different cognitive biases have been identified in healthcare settings, and the overall rate of incorrect diagnosis has been estimated to fall between 10% and 15%. These aren’t abstract academic curiosities. A systematic review found that cognitive bias contributed to diagnostic errors in 36% to 77% of studied physician case scenarios. The same flawed cognitive machinery that warps clinical judgment also distorts how you remember your own year — the wins you dismiss, the growth you overlook, the balance you’ve actually achieved but refuse to believe in.
Which is precisely why the year-end reflective review isn’t a soft exercise in journaling. It’s a corrective lens for a mind that cannot be trusted to assess itself without structure.
Why Reflection Is No Longer Optional
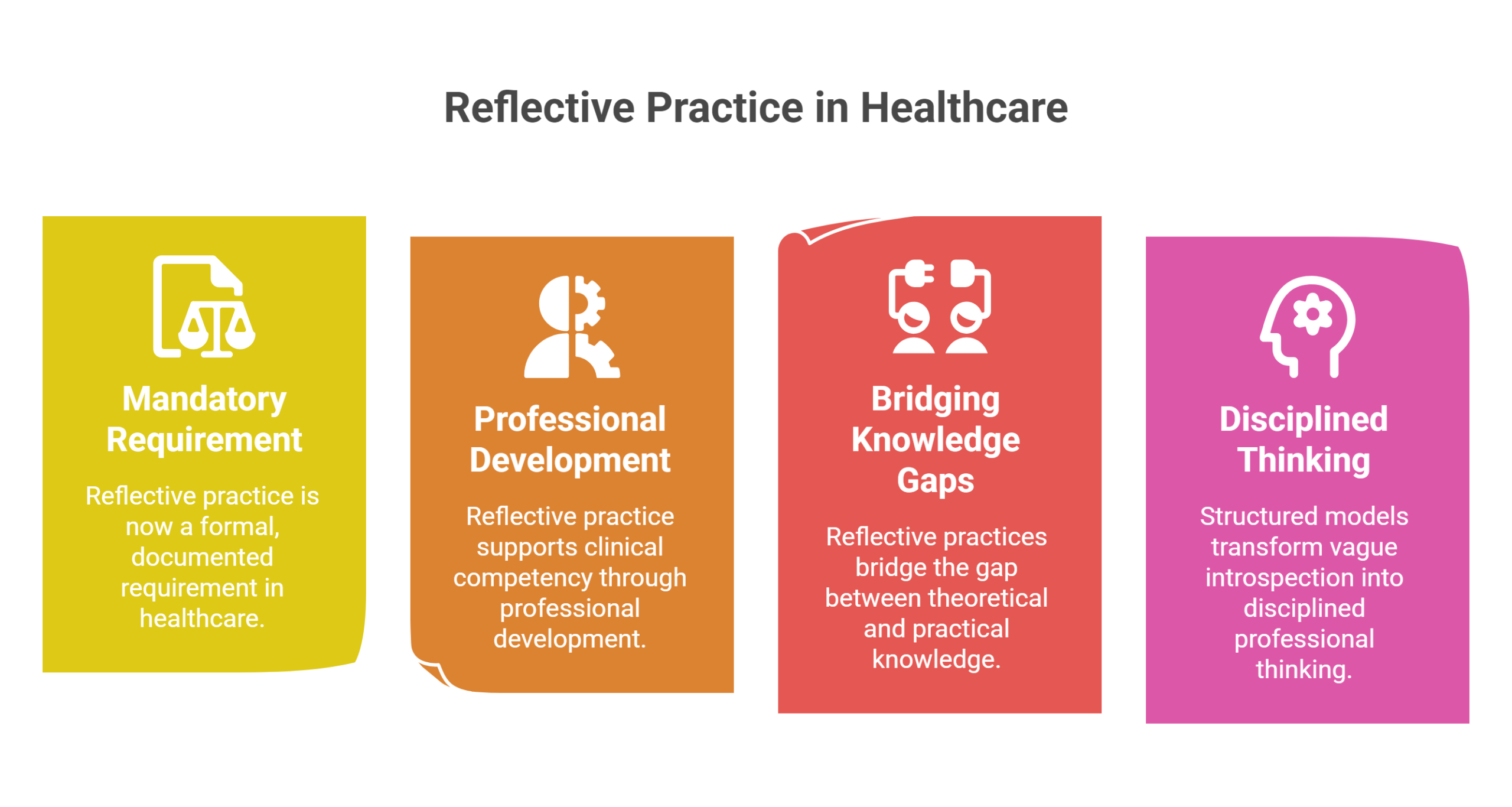
Reflective practice in healthcare has evolved from a vaguely encouraged habit into a formal, documented requirement. Professionals are now expected to provide evidence of their reflections through training portfolios and throughout their career in revalidation processes. In 2018, the General Dental Council in the UK made a reflective element mandatory for all registrants in its Enhanced Continuing Professional Development system. Professional organizations and regulatory bodies worldwide are making critical reflection a mandatory component of professional practice.
This isn’t bureaucratic theater. Among 13 studies examined in a recent scoping review, reflective practice was found to be beneficial for supporting clinical competency through professional development. The research showed that reflective practices bridge the gap between theoretical and practical knowledge while encouraging self-discovery and self-awareness. Across disciplines, structured models — Gibbs’, Schön’s, Kolb’s, Johns’, and Mezirow’s frameworks — provide the scaffolding that transforms vague introspection into disciplined professional thinking used across nursing, medicine, and pharmacy.
Your Mind Is Not a Reliable Narrator
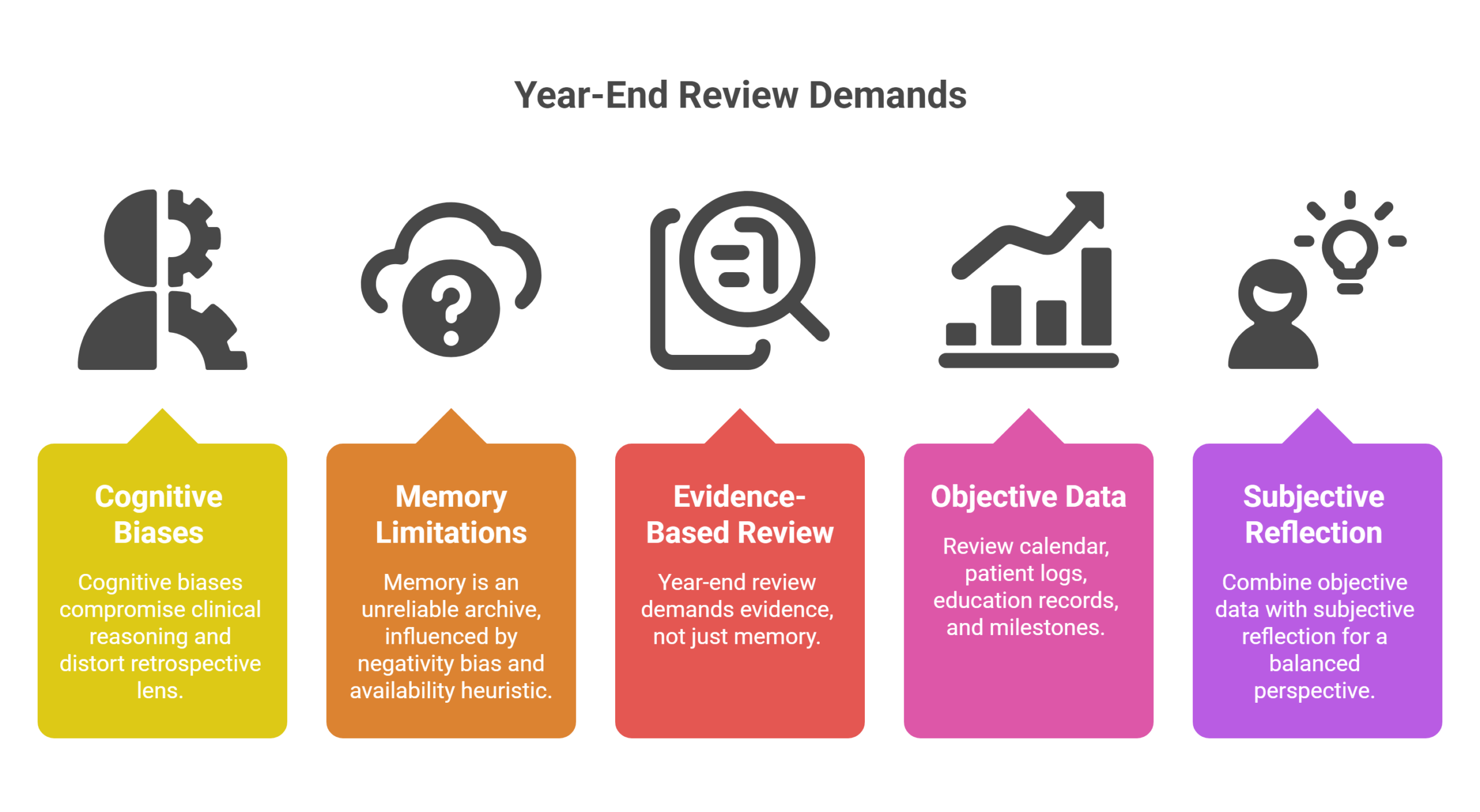
The same cognitive biases that compromise clinical reasoning in anaesthesia and intensive care don’t clock out when you turn your gaze inward. You may believe you were less present for your family than you actually were. You may dismiss a year of steady growth because one difficult quarter looms disproportionately large. The negativity bias, the availability heuristic, confirmation bias — they all distort the retrospective lens.
This is why the year-end review demands more than memory. It demands evidence. Review your calendar. Revisit your patient logs, your continuing education records, your documented milestones. Combine objective data with subjective reflection — not because feelings don’t matter, but because feelings alone are an unreliable archive.
Reflection as a Debiasing Tool — With a Caveat
The promising news: guided reflection works. Resident clinicians who used reflective practice made more correct diagnoses than those who did not — 52% versus 43%. Cognitive forcing strategies and guided reflection deflect bias through close examination of our own thinking processes.
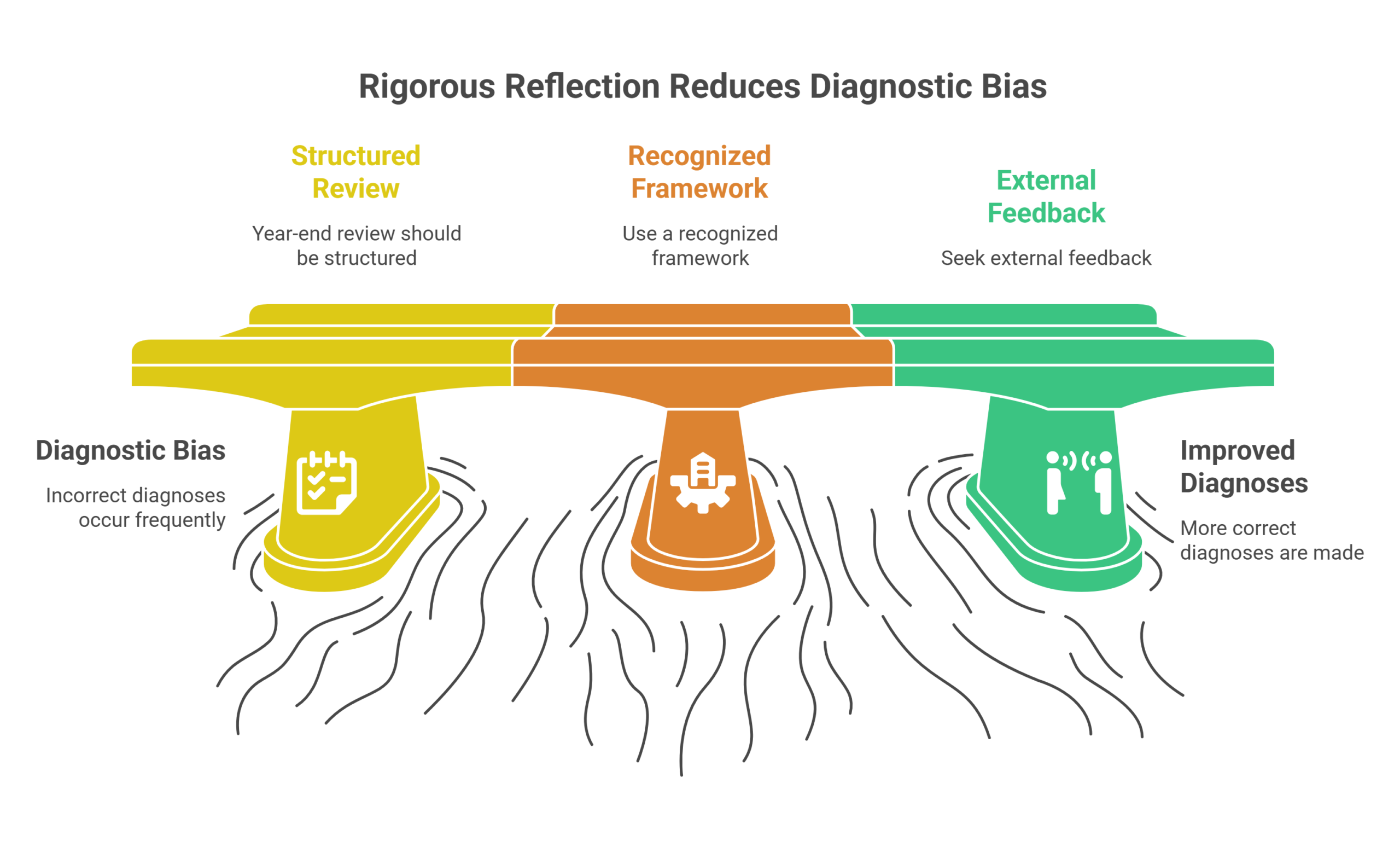
The honest caveat: most proposed strategies for reducing bias rely on the ability of an imperfect cognitive system to check itself. The great majority of these strategies are promoted based on opinion rather than rigorous evidence. This doesn’t invalidate the practice — it sharpens it. It means your year-end review should be structured, not freeform. It means using a recognized framework rather than simply sitting with your thoughts. And it means, wherever possible, seeking external feedback to complement your self-assessment.
The evidence for reflection’s contribution to clinical practice, while broadly supported, remains partly theoretical. That’s not a reason to abandon it. It’s a reason to do it with rigor rather than ritual.
A Practitioner’s Year-End Protocol
- Gather the evidence. Review your professional calendar and records from January through December. Document patient interactions, procedural milestones, continuing education, and collaborative engagements.
- Identify the high moments. Look for groundbreaking clinical achievements, successful interventions, new skills, mentorship experiences, and improved work-life integration. Don’t overlook the quiet victories.
- Challenge the narrative. Where does the objective record contradict your felt sense of the year? Use data to correct distortions — not to dismiss your emotions, but to complete the picture.
- Extract the patterns. Which activities brought professional purpose? What elevated your sense of identity as a healthcare provider? What, if expanded, could deepen both performance and satisfaction?
- Build forward deliberately. Schedule time for what matters. Fulfilling experiences do not happen by accident — they are engineered through intentional planning and coordination with colleagues and loved ones.
The year you think you had is a rough draft written by a biased author. The year you actually lived is recoverable — but only through disciplined, structured, evidence-informed reflection. In a profession where the margin between good and great is often a matter of awareness, the most consequential diagnosis you’ll make this December is the one you make about yourself.
Sources: PubMed Central (NIH) · ScienceDirect · AMA Journal of Ethics · Tandfonline · MDPI




{kind=link}
{kind=link}
{kind=link}